Following a decade of effective front line delivery in South Wales the rest of Wales needs to step up and support this vital service
In a decade, 5,135 patients – primarily women – were identified as survivors of domestic abuse and referred for support through IRIS. It is incomprehensible that the model has not become mainstream everywhere. Click here to download and read our infographic.
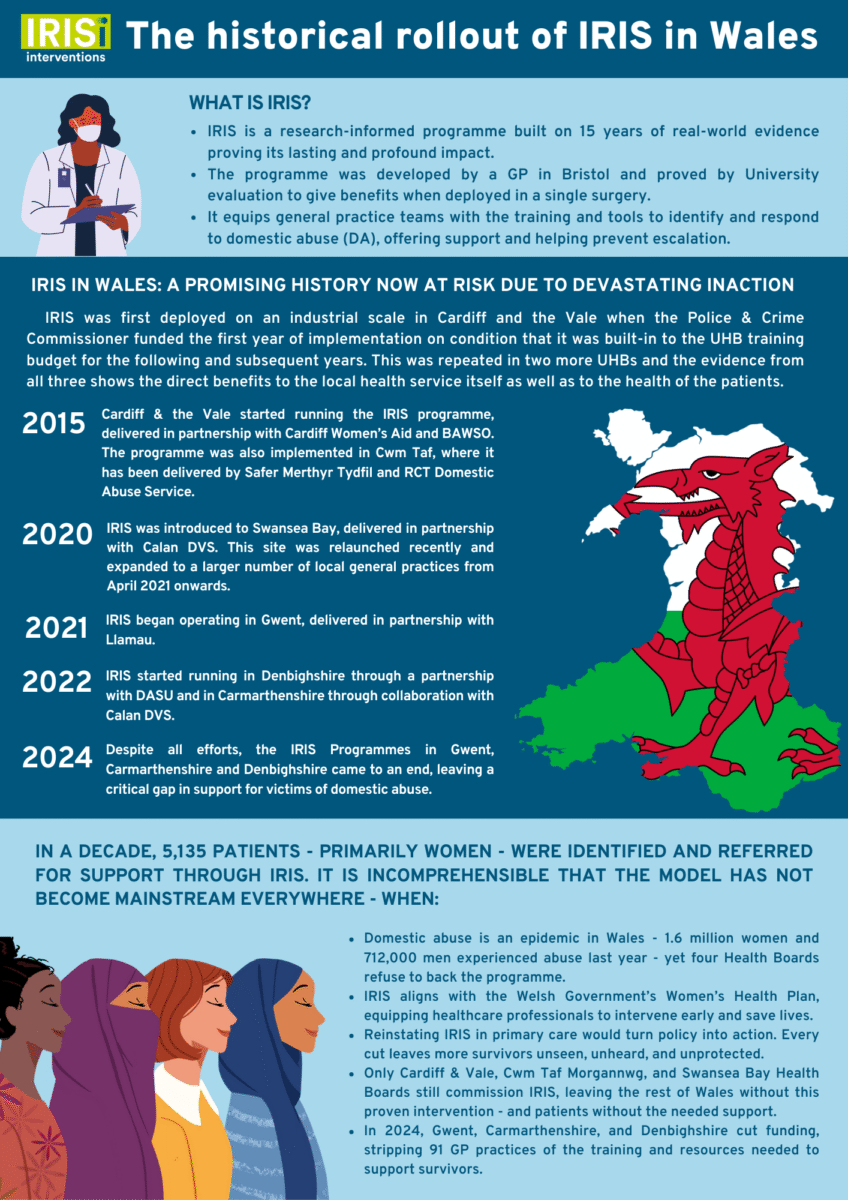
In 2015, funding from the Police and Crime Commissioner (PCC) for South Wales enabled Cardiff and Vale University Health Board to become the first in Wales to implement IRIS — Identification and Referral to Improve Safety. The programme trains GP teams to recognise domestic abuse and refer patients to specialist support, creating a new frontline in healthcare’s response. Delivered in partnership with Cardiff Women’s Aid and BAWSO, the pilot proved both popular and effective. Within a year, the Health Board absorbed IRIS into its core training and budget.
The same model — with initial costs again met by the PCC — led to adoption in the other two South Wales Health Boards: Cwm Taf Morgannwg, where the programme began to be delivered in partnership with Safer Merthyr Tydfil and RCT Domestic Abuse Services, and Swansea Bay, in partnership with Calan DVS.
The success in South Wales set the tone for what followed. Eventually, IRIS expanded across six of the seven health boards in the country, each delivered in partnership with trusted local organisations and supported by a mix of funders: Gwent (Llamau, funded by Neighbourhood Care Networks, NCNs), Carmarthenshire (Calan DVS, funded by Hywel Dda UHB), and Denbighshire (DASU, funded through a limited pilot supported by Betsi Cadwaladr UHB).
From pilot to proven success
The IRIS model quickly proved its worth. In Cwm Taf Morgannwg, where only four primary care referrals had been made prior to implementation, the number surged to over 1,450 by January 2025. In Cardiff & Vale, referrals reached 2,115. Swansea Bay, which relaunched its programme in October 2022 after an initial funding gap, recorded 550 referrals. Gwent logged over 1,020 between July 2021 and March 2024. In total, more than 5,135 survivors across Wales were identified and referred for support in just ten years.
The model’s impact stretched beyond numbers. Survivors in Gwent reported 100% satisfaction with the service, with 80% saying they felt safer, more able to cope, and more optimistic. In Cwm Taf Morgannwg, 100% of patients reported being pleased to be asked about safety by their GP or nurse, and 100% felt that the support they received was helpful.
A sharp U-turn in 2024
Despite its proven success, 2024 brought a wave of decommissioning. Four of Wales’s seven health boards – Gwent, Carmarthenshire, Denbighshire, and Betsi Cadwaladr – withdrew funding, dismantling IRIS across more than 140 GP surgeries and leaving 91 practices without any referral infrastructure to support survivors.
In Gwent alone, the decision ended a service that had been building steadily through local investment and strong clinical engagement. Denbighshire and Carmarthenshire, where IRIS had not yet reached scale, also terminated their programmes, cutting off promising developments. In Swansea Bay, by contrast, the health board stepped in after initial PCC funding to expand the model. Only Cardiff & Vale, Cwm Taf Morgannwg, and Swansea Bay continue to commission IRIS today.
Meeting survivors where they already are
At the heart of IRIS is a principle rooted in trust: nearly every woman will visit her GP at some point. That encounter, often in a safe and private setting, can be the moment she discloses abuse. The discretion of the GP setting makes it uniquely powerful.
This is especially critical given the gendered nature of domestic abuse. According to the Crime Survey for England and Wales, an estimated 2.3 million people aged 16 and over experienced domestic abuse in the year ending March 2024. Of these, 1.6 million were women and 712,000 were men, making women more than twice as likely to be affected.
With women disproportionately affected – and often less likely to have the confidence to engage with criminal justice routes – the GP consultation becomes a vital point of access. IRIS ensures that when survivors walk through the surgery door, they enter a system designed to listen, respond and protect.
“Some fled abuse decades ago and only now feel the impact”, said Shaheena Chowdhury and Parnaz Hussain of BAWSO, who support the Cardiff & Vale rollout. “We’ve had referrals from women in their eighties. IRIS fills that gap. It’s not just for people at immediate high risk; we’re here for medium and lower-risk cases too, offering continued support and preventing things from escalating”.
Giving GPs the tools to act
Clinicians also report dramatic change. “Before IRIS, they’d sit in front of a patient and know something was wrong, but they didn’t know what to do, there were no clear referral pathways to support victims in need”, said Mark Gall, former Deputy Manager for Primary Care in Cwm Taf Morgannwg. “IRIS was a fix. A discreet, effective fix”.
Dr Jacqueline Gantley, former GP and clinical lead for IRIS in South Wales, saw the difference too. “Those patients started coming in less often. Someone had finally listened. Someone had offered proper support.”
IRIS made primary care safer, more responsive, and more efficient across Wales. It helped survivors to be heard, while enabling clinicians to know exactly what to do.
When the evidence exists, but the funding doesn’t
In July 2025, the UK Government announced a £53 million national rollout of DRIVE, a programme focused on perpetrators which has been driven effectively across South Wales by the PCC’s team. While the UK roll-out has been widely welcomed, leaders in Wales stressed that DRIVE cannot and must not replace IRIS.
“We need both schemes: IRIS for survivors, and DRIVE for perpetrators”, said Rt Hon Alun Michael, who as Police & Crime Commissioner for South Wales funded the original Cardiff launch. “Our top priority was to help the victims and stop domestic violence being a hidden crisis. But we recognised that many perpetrators are serial offenders – so we leaped at the opportunity to pilot the DRIVE approach as well. When the initial DRIVE grant funding ran out in March 2020, I and the chief constable agreed that we couldn’t allow it to lapse – so instead of dropping the approach in the two pilot areas we committed to expanding the service across the seven local authority areas (three health board areas) in our region. But this was not instead of supporting survivors, it was in addition to our support for IRIS and complementary to IRIS. That balance matters”.
The IRIS model is backed by a decade of evaluation. Yet instead of expansion, Wales has witnessed retreat. In December 2024, the Welsh Government published its long-awaited Women’s Health Plan. The strategy acknowledged domestic abuse and committed to better training and research. But there was no funding attached and no pathway for embedding IRIS into the plan.
“These brilliant policy announcements are made, but there’s no funding attached”, said Dr Gantley. “The plan’s there, but where are the resources?”. The result is clear: GPs who want to help survivors have no referral route. Clinicians and team members who have a chance to listen to survivors are left without tools. And a decade of progress is being undone in the health boards that have abandoned IRIS.
The future is still unwritten
As IRIS marks ten years in Wales, it stands as a rare example of what survivor-centred, evidence-led healthcare can achieve. The question is no longer whether IRIS works; It does. The question is whether Wales will invest in keeping it working.
That investment is not only a moral imperative but a policy one. In a recent interview, Jess Phillips MP, Parliamentary Under-Secretary of State for Safeguarding and Violence Against Women and Girls, underlined the need for evidence-based decisions: “I have to look at the evidence of what is actually going to work.”
The evidence for what works in primary care already exists. It’s IRIS.
- It is 4.8 times more cost-effective than the flu jab.
- It delivers a £16.79 return for every £1 invested.
- Its social return is £10.71.
- It has reached thousands of women across the UK, many of whom had never disclosed abuse before.
- And it has transformed the way GPs respond to one of the most widespread public health issues of our time.
Yet instead of scaling it up, Wales saw decommissioning.
The call to Welsh Government for action is clear: reinstate IRIS in every health board and expand it to fully cover every practice in every part of Wales. Make it the national standard it was always meant to be. And embed it fully into the Women’s Health Strategy, not as an afterthought, but as a cornerstone of prevention.
“IRIS fills the gap”: what frontline voices say makes this programme unlike any other
If you ask those who’ve delivered IRIS on the ground, they won’t speak of a programme, they’ll speak of a lifeline.
For Shaheena Chowdhury and Parnaz Hussain, Advocate Educators at BAWSO, the benefit to GPs is clear. “Many were overwhelmed before. They’d sense something was wrong with their patients but didn’t know what to do. Now, the process is quick; it’s just a form. It takes two seconds. And we’re reducing GP appointment times. Survivors feel heard, supported, and they stop returning again and again without their real issues being addressed”.
The team also point to the ways IRIS quietly but effectively lifts pressure off the wider health system. By identifying survivors earlier and offering immediate specialist support, the model prevents repeated visits for the same underlying issue. Critically, “IRIS is there for survivors who don’t fit crisis thresholds – those living with trauma years after fleeing abuse, or whose experiences don’t meet the high-risk markers that trigger other interventions”.
Crucially, it doesn’t just empower GPs themselves to help, but all their team members – nurses and reception staff in particular – and everyone can help. Two thirds of those who have been helped via IRIS had never previously disclosed the abuse, not even to a close family member. Staff are empowered and survivors can speak to someone they trust.
That foundation of trust is key, said Mark Gall, former Deputy Manager for Primary Care in Cwm Taf Morgannwg. “We’ve already got a proven system, a structure that works in general practice”, Mark explains. “Even A&E departments are sending patients back to their GPs with safeguarding flags. Social workers know about IRIS. What we need now is some joined up thinking across all sectors of Health and Social Care to make the whole process more streamlined, because the model works”.
“It’s also about public services cooperating with each other – to the benefit of both as well as the public they both exist to serve”, says Alun Michael. “I’m fond of saying that ‘everything is connected to everything else’ because its true: Domestic violence is one of the worst scandals of our time and whenever we tackle it and reduce it we help to improve the lives of the survivors, their families, their community, but we also reduce demand on the NHS – particularly GP surgeries – and on the police and the local council. That’s why it was supported so strongly from the start by Jane Hutt as our lead Minister for tackling the issue in Wales. The failure to implement IRIS effectively in four of seven Welsh Health Boards is a national scandal”.
Dr Jacqueline Gantley, who led IRIS as a Clinical Lead in Cwm Taf Morgannwg, says it goes beyond referrals. “The truth is, IRIS is not just another referral system. It’s about transforming the way primary care responds to violence against women and girls. And it works, because it’s rooted in trust, built for the real world of general practice, and designed with survivors in mind.”


